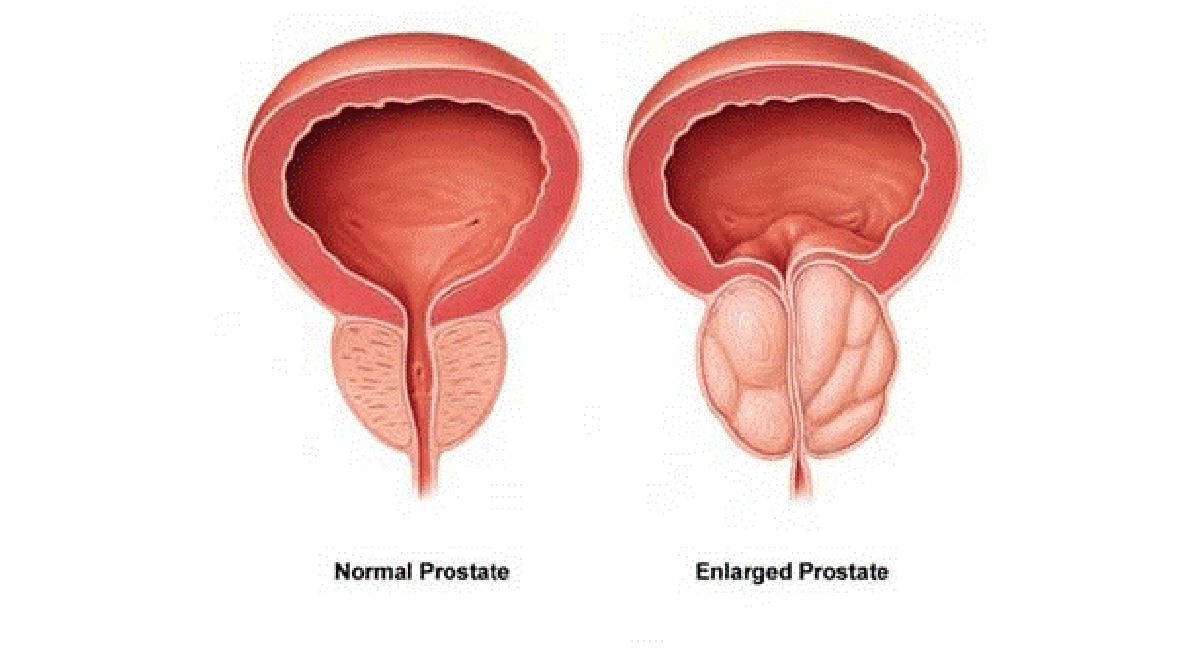
BPH is a non-cancerous condition where the prostate gland grows larger, according to the National Cancer Institute (NCI). The prostate is located below the bladder and surrounds the urethra, the tube that carries urine out of the body.
Common symptoms of BPH include:
- Frequent or urgent need to pee, also called urination.
- Peeing more often at night.
- Trouble starting to pee.
- Weak urine stream, or a stream that stops and starts.
- Dribbling at the end of urination.
- Not being able to completely empty the bladder.
- Urinary tract infection.
- ot being able to pee.
- Blood in the urine.
The symptoms of BPH tend to slowly get worse. But sometimes they stay the same or even improve over time.
The size of the prostate doesn't always determine how serious the symptoms are. Some people with slightly enlarged prostates can have major symptoms. Others who have very enlarged prostates can have minor problems. And some people with enlarged prostates don't have any symptoms at all.
The prostate gland is located beneath the bladder. The tube that moves urine from the bladder out of the penis is called the urethra. This tube passes through the center of the prostate. When the prostate gets bigger, it starts to block urine flow.
The prostate is a gland that typically keeps growing throughout life. This growth often enlarges the prostate enough to cause symptoms or to block urine flow.
It isn't clear what causes the prostate to get bigger. It might be due to changes in the balance of sex hormones as you grow older.
BPH severe enough to cause troublesome urinary symptoms is common in older men. Age seems to be the primary risk factor. It's rare in men age 40 and younger, but half the men in their 60s have BPH symptoms. These symptoms generally worsen with age. Up to 90 percent of men in their 70s and 80s have prostate gland enlargement. A family history of BPH slightly increases your chances for the condition.
Risk factors for an enlarged prostate include:
Aging: An enlarged prostate gland rarely causes symptoms before age 40. After that, the chance of having an enlarged prostate and related symptoms starts to rise.
Family history: Having a blood relative with prostate problems makes you more likely to have problems with your prostate.
Diabetes and heart disease: Studies show that diabetes might raise the risk of BPH. So maybe heart disease.
Lifestyle: Obesity raises the risk of BPH. Exercise can help lower the risk.
Complications of an enlarged prostate can include:
Not being able to pee: This is also called urinary retention. You might need to have a tube called a catheter placed into your bladder to drain the urine. Some people with an enlarged prostate need surgery to get relief.
Urinary tract infections (UTIs): Not being able to fully empty the bladder can raise the risk of infection in the urinary tract. If you often get UTIs, you might need surgery to remove part of the prostate.
Bladder stones: These are most often caused by being unable to fully empty the bladder. Bladder stones can cause illness, bladder irritation, blood in the urine and blocked urine flow.
Bladder damage: A bladder that doesn't empty fully can stretch and weaken over time. As a result, the muscular wall of the bladder no longer squeezes properly to force urine out. And this makes it harder to completely empty the bladder.
Kidney damage: Pressure in the bladder from not being able to pee can damage the kidneys or let bladder infections reach the kidneys.
Treatment for BPH lowers the risk of these complications. But urinary retention and kidney damage can be serious health threats.
Having an enlarged prostate is not thought to raise the risk of getting prostate cancer.
To diagnose BPH, your doctor will review your medical history and do a physical exam and then may arrange for you to have one or more tests.
As a rule, the shorter the stricture, the greater the chance of a cure with dilation. It is a relatively easy procedure to do and so may be tried first.
History: Symptoms you are having, including difficulty in passing urine, stream, frequency, etc. Digital rectal exam. Wearing a lubricated examination glove, your doctor gently inserts a finger into your rectum. Your doctor checks the size, texture and shape of the gland. This allows your doctor to determine whether your prostate is enlarged and to help rule out prostate cancer.
Urine test: Analyzing a sample of your urine in the laboratory can help rule out an infection or other conditions that cause BPH-like symptoms, such as temporary inflammation of the prostate (prostatitis), bladder infection and kidney disease.
Tests your doctor may use to help confirm BPH diagnosis:
Symptom questionnaire: The American Urological Association (AUA) BPH Symptom Score Index asks you how severely and how frequently you have specific urinary symptoms. It's one way to monitor if your symptoms are getting worse over time. You can check your urinary symptoms by completing the Prostate symptoms self-assessment.
Prostate-specific antigen (PSA) blood test: It's normal for your prostate gland to produce PSA, which helps liquefy semen. A small amount of PSA normally circulates in your blood. Higher than normal levels in your blood can indicate you have BPH, prostate cancer or prostatitis. Most physicians use this test in men with BPH to be sure that a hidden prostate cancer isn't missed.
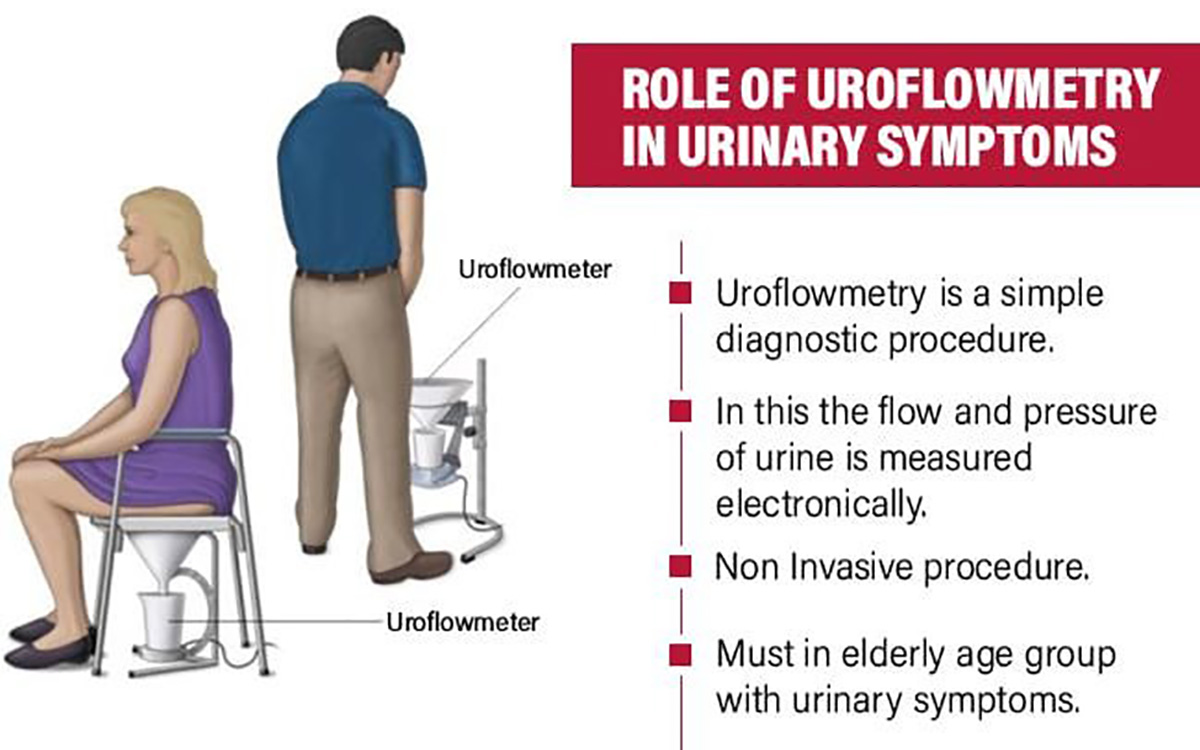
This test measures the strength and amount of your urine flow. You urinate into a receptacle attached to a special machine. The test takes no longer than a normal urination. Charting the results of this test over time helps determine if your condition is getting better or worse. It's normal for peak urine flow to decrease with age, but it can also be a sign of BPH or a weakened bladder muscle. After passing urine, your residual urine is checked on an ultrasound machine.
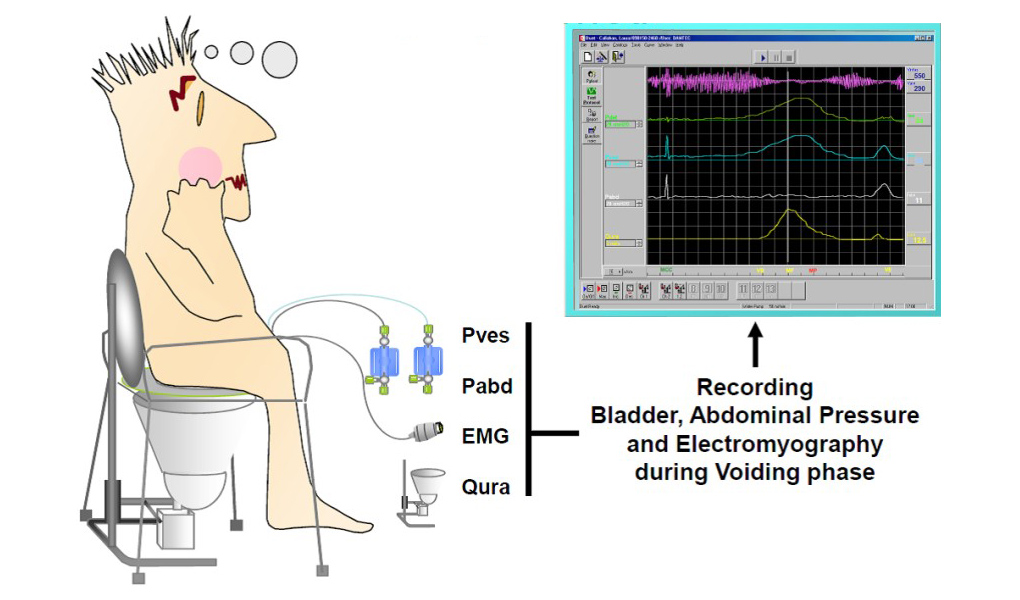
Urodynamic pressure-flow studies: This test measures bladder pressure and function while you urinate. After you receive a local anesthetic, a small catheter is threaded through your urethra into your bladder. Water is slowly injected into your bladder to measure internal bladder pressure and to determine how effectively your bladder contracts. Bladder pressure and urinary flow may be measured while you urinate. The test takes 30 to 60 minutes. Generally, this test is reserved for men with complicated or unusual urinary symptoms.
Most men who seek treatment do so because they're bothered by lower urinary tract symptoms. All BPH treatments attempt to reduce the severity of symptoms and restore the normal function of the urinary system. Different treatments provide different degrees of relief. How severe your symptoms are and how bothered you are by them are key to deciding which treatment option is best for you. Depending on how large your prostate is, and the location of excess prostate tissue, some treatment options may be more appropriate than others.
- Watchful Waiting
- Lifestyle changes to reduce symptoms
- Medicines
- Surgery
- Transurethral resection of the prostate
- Transurethral incision of the prostate
- Open prostatectomy
- Pros and cons of surgery
Medications are the most common way to control mild to moderate symptoms of BPH. They're the preferred way to treat BPH, unless your condition is severe enough to require surgery. Medications significantly reduce major symptoms for about two-thirds of men who try them. If medications don't work, a minimally invasive treatment or surgery may be the best option.
Two types of medications currently used to treat BPH are Alpha Blockers and enzyme inhibitors. Alpha blockers relax muscles around the neck of your bladder, which makes it easier for urine to flow through your urethra. Enzyme inhibitors shrink the size of your prostate gland. Sometimes the two types of drugs are prescribed in combination.
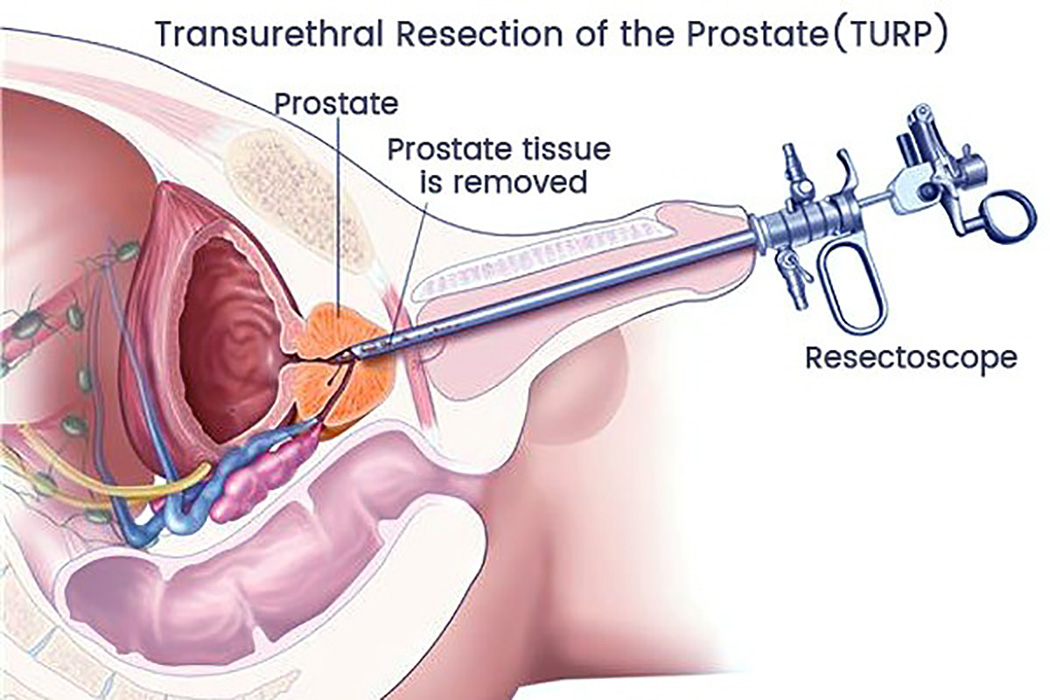
Transurethral resection of the prostate (TURP) is a procedure frequently used to treat moderate to severe BPH. It was one of the most common major surgeries performed on men age 65 and older but is rapidly being replaced by laser prostatectomy and other less invasive procedures.
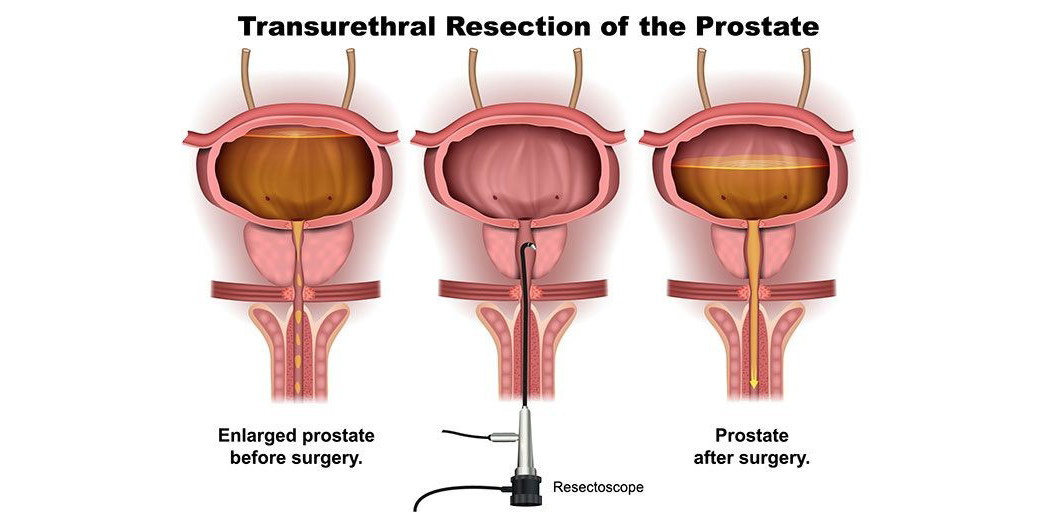
After you're given a spinal or general anesthetic, an instrument called a resect scope is inserted into your urethra through your penis.
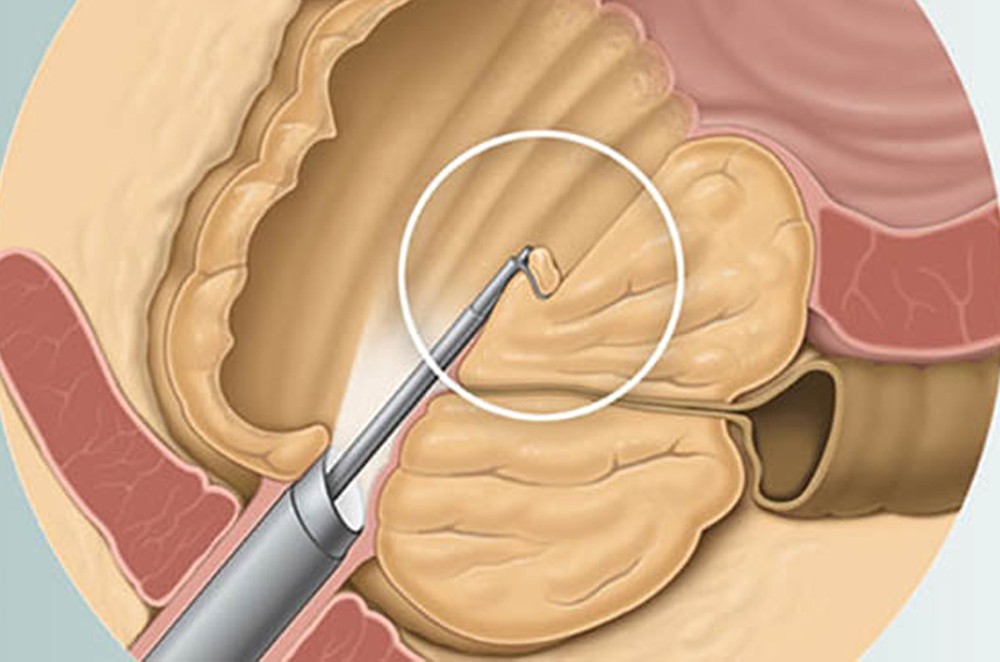
During the 60 to 90 minute operation, your surgeon uses the scope's wire loop to remove obstructing tissue one piece at a time from the inside of your gland, creating a cavity. Only the interior part of your gland is removed. This tissue is carried by the irrigating fluid into the bladder, and then flushed out at the end of the operation. Expect some blood or small blood clots in your urine afterward. You'll probably need a urinary catheter for a few days. At first, you may have painful urination or a sense of urgency as urine passes over the surgical area. This gradually improves over one to four weeks. You can go back to office work in about two weeks and back to manual labor in four to six weeks. You can resume sexual activity in four to six weeks.
TURP greatly relieves lower urinary tract symptoms in nearly all men. It produces the greatest symptom relief in men who have larger prostate glands and more troublesome symptoms. Even men with severe bladder damage caused by BPH often improve after TURP.
TURP relieves symptoms quickly. Most men experience a stronger urine flow within a few days.
TURP can cause excessive bleeding, although this is rare with modern surgical techniques. Frequent urge to urinate is common during the early recovery period, but is rare long term with about the same frequency as occurs in men who choose watchful waiting.
TURP syndrome occurs when your bloodstream absorbs too much of the irrigating solution, causing abnormally low concentrations of sodium in your blood. It rarely occurs anymore due to current surgical techniques and is readily treated.
Prolonged side effects of TURP may include:
- Semen entering your bladder (retrograde ejaculation)
- Erection problems
- painful urination
- Recurring urinary tract infections
- Bladder neck narrowing (stricture)
- Blood in your urine (hematuria)
Later treatment after TURP is uncommon and significantly less likely, compared with minimally invasive treatments. Some men may need a second surgery after a number of years. A few men require re-treatment because their prostate gland regrows or because not enough of it is removed the first time. Newer Tequniqes like HOLAP, HOLEP, HOLRP are more effective & durable.
Holmium Laser Enucleation of the Prostate (HoLEP)
© 2025 Om Kidney Hospital. All Rights Reserved. Designed & Developed By: Desiration Hub.
