Stress Urinary incontinence is a common problem in later age. We have done successfully bladder neck & mid urethral suspension surgery by T-Suit, TOT - Transobturotor mid urethral sling surgery. Other patient can be treated medically.
We do cystoscopy, uroflowmetry & complete urodynamics workup for patient of voiding difficulties.
We treat patient of recurrent UTI
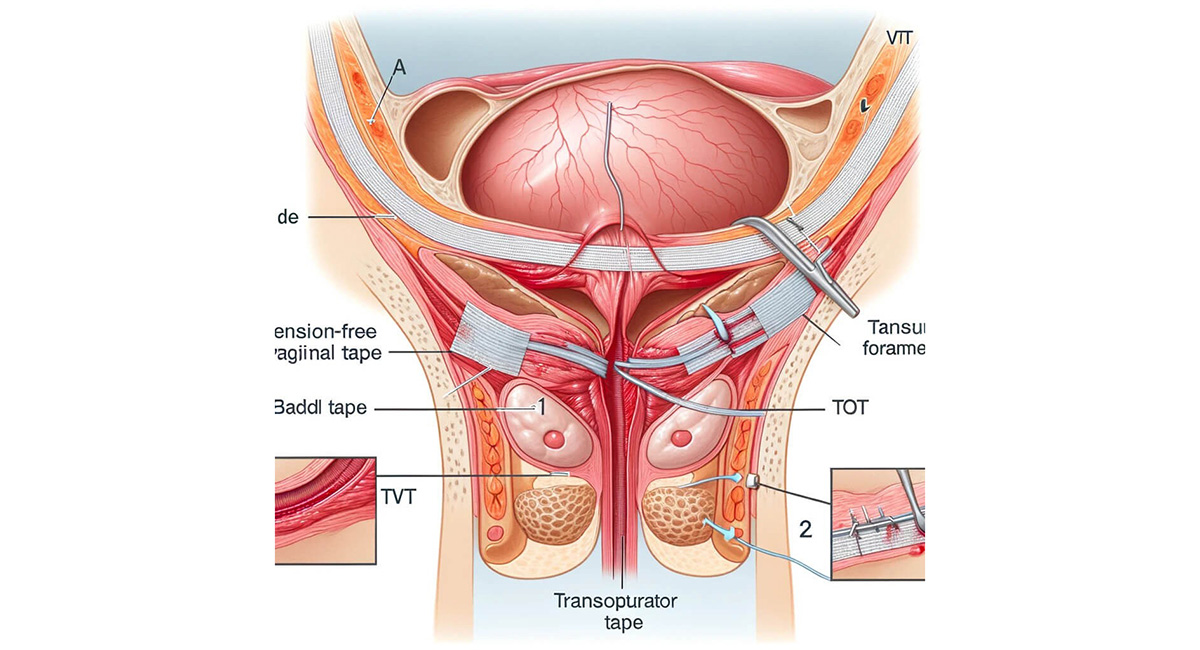
TOT (Trans-Obturator Tape) surgery is a procedure to treat urinary incontinence, specifically stress incontinence, where urine leaks when there is pressure on the bladder. It involves placing a synthetic mesh sling to support the urethra, helping to prevent urine leakage. The surgery is performed by making small incisions and passing a needle and tape through the obturator foramen, a space in the pelvis.
The steps for a percutaneous nephrolithotomy are as follows:
Day care procedure
Minimally invasive
Nearly painless
Durable
Urinary incontinence in females is a loss of bladder control, leading to involuntary leakage of urine. It is a common but often underreported condition that affects women of all ages, especially after childbirth, during menopause, and in older age.
Women experience incontinence twice as often as men. Pregnancy and childbirth, menopause, and the structure of the female urinary tract account for this difference. But both women and men can become incontinent from neurologic injury, birth defects, strokes, multiple sclerosis, and physicalproblems associated with aging.
Older women, more often than younger women, experience incontinence. But incontinence is not inevitable with age. Incontinence is treatable and often curable at all ages. If you experience incontinence, you may feel embarrassed. It may help you to remember that loss of bladder control can be treated. You will need to overcome your embarrassment and see a doctor to learn if you need treatment for an underlying medical condition.
Incontinence in women usually occurs because of problems with muscles that help to hold or release urine. The body stores urine water and wastes removed by the kidneys in the bladder, a balloon-like organ. The bladder connects to the urethra, the tube through which urine leaves the body.
During urination, muscles in the wall of the bladder contract, forcing urine out of the bladder and into the urethra. At the same time, sphincter muscles surrounding the urethra relax, letting urine pass out of the body. Incontinence will occur if your bladder muscles suddenly contract or muscles surrounding the urethra suddenly relax.
Cause: Weak pelvic floor muscles.
Trigger: Coughing, sneezing, laughing, exercising.
Common in: Women post-childbirth or post-menopause.
Cause: Overactive or irritated bladder muscles.
Symptom: Sudden intense urge to urinate followed by involuntary leakage.
Common in: Older women.
Combination of stress and urge incontinence.
Symptoms: Leakage during physical activity and strong urge to urinate.
Cause: Incomplete bladder emptying due to weak bladder muscles or blockage.
Symptom: Frequent dribbling or constant leakage.
Less common in women.
Cause: Physical or mental barriers that prevent reaching the toilet in time.
Examples: Arthritis, dementia.
Less common in women.
Pregnancy and childbirth
Menopause (estrogen deficiency affects tissue tone)
Pelvic surgery (e.g., hysterectomy)
Aging
Obesity (increases bladder pressure)
Chronic cough or constipation
Neurological disorders (e.g., MS, Parkinson’s)
Urinalysis (infection or blood)
Bladder diary (record frequency, volume, and leakage)
Pad test (measure urine leakage)
Post-void residual volume (check incomplete emptying)
Urodynamic testing (measure bladder pressure and flow)
Pelvic ultrasound or cystoscopy (in selected cases)
Pelvic Floor Exercises (Kegels)
Bladder training (scheduled voiding)
Lifestyle changes
Weight loss
Reduce caffeine/alcohol
Treat constipation
Absorbent pads and protective garments
Pessary (for pelvic organ prolapse)
Urethral inserts (temporary devices to prevent leakage)
Mid-urethral sling surgery (common for stress incontinence)
Bladder neck suspension
Bulking agents (injected into the urethra)
Botox injections (for overactive bladder)
Sacral nerve stimulation
With proper diagnosis and treatment, most women experience significant improvement. Long-term results are best with a multidisciplinary approach combining physical therapy, medication, and sometimes surgery.
Do regular Kegel exercises
Maintain a healthy weight
Avoid smoking (chronic cough weakens pelvic floor)
Manage chronic constipation
Stay physically active
© 2025 Om Kidney Hospital. All Rights Reserved. Designed & Developed By: Desiration Hub.
